Franz W. Gatzweilera, 1 and Philippa Howden-Chapmanb, 2
a. Institute of Urban Environment, Chinese Academy of Sciences
b. University of Otago, Wellington, New Zealand
Abstract
Cities of the future will need to cope with the triple challenges of urban growth, planetary boundaries leading to reduced energy and other resources, and rapid climate change. In response to the challenges of these complexities, urban growth and innovations in networked infrastructure development need to go hand-in-hand to transform urban systems and sustain the urban health advantage. In order to achieve this, knowledge and policy-making need to undergo processes of accelerated learning. The International Science Council’s global science programme “Urban Health and Wellbeing: A Systems Approach” has formulated goals to meet the urban health challenges of future cities.
Cite this article as
Gatzweiler, F.W. and Howden-Chapman, P. (2022) A New Interdisciplinary Science Plan for Urban Health and Wellbeing in an Age of Increasing Complexity. Bulletin of the Chinese Academy of Sciences, 36(2), 21–26. DOI: https://doi.org/10.1051/bcas/2022001
Introduction
In 2002, the International Science Council, first recognised health as an important focus for science. The first science plan was then submitted to its General Assembly in 2011. The science plan of 2011 laid out the vision and key concepts of the programme and the importance of a systems approach to better understanding health and wellbeing in the rapidly changing urban environments. It was then decided to establish a new global science programme which would take a systems approach to urban health and wellbeing. The programme was established at the Institute of Urban Environment of the Chinese Academy of Sciences and took up its global operations in October 2014.
The new science plan deviates from its 2011 predecessor by making a shift from “improving health and wellbeing of people in cities” to “improving population and planetary health in the context of complex urban systems”. It focuses on the interactions of people with the environment in complex urban systems, with health resulting as an emergent systemic property. While both plans have applied systems thinking, the difference between the previous and the new approaches lies in the recognition that in the age of the Anthropocene, a less anthropocentric and more eco-centric view becomes necessary (Küpers, 2020; Kotzé and French, 2018).
Highlighting the urgency of this shift, in the decade between the first and the second science plans, the adverse trends of many planetary and human health symptoms have continued, including the COVID-19 pandemic – which has made accelerated learning for health and wellbeing by applying a systems approach even more urgent than before. The COVID-19 pandemic has starkly revealed the systemic nature of urban health (Gatzweiler et al., 2020) and has further widened existing social and economic inequalities in many cities, making the virus more harmful beyond its direct detrimental human health impacts.
As the recent COVID-19 pandemic has demonstrated, the interlinkages, synergies, trade-offs and feedbacks between human systems and environmental systems in a rapidly urbanising world make an integrated systems approach for human and planetary health necessary (Thoradeniya and Jayasinghe 2021). Cities are neural centres where many challenges emerge, but also where the foresight, planning and decision-making on how to address them can be made and implemented.
In this article, the context, challenges, opportunities, goals and proposed actions of the new science plan for urban health and wellbeing, are presented in brief. They have been elaborated by the scientific committee of the Urban Health and Wellbeing (UHWB) programme and aim at guiding urban health related decision making and initiatives in cities of all regions of the world.
Context and Challenge
In the last decade, the trends in planetary and human health have continued, often at an exponential rate, and imposed additional pressures on people and the planet. Deforestation and fossil fuel burning have increased CO2 levels in the Earth’s atmosphere from 280 ppm in preindustrial times to over 400 ppm today, causing a rise in the Earth’s surface temperature. Despite international agreements, greenhouse gas emissions have doubled since 1980 and continue to rise (IPCC, 2018). The 6th Intergovernmental Panel on Climate Change (IPCC) assessment report (2021) issued a “code red for humanity” with increasing extreme weather events as well as occurrences of interconnected risks like sea level rise, food security, health, and biodiversity loss.
While cities have largely been associated with the “urban advantage” of better infrastructure and public service provisions, such as education and healthcare, emerging and fast-growing cities in Sub-Saharan Africa can be turning that advantage into an “urban penalty”. Antai et al (2010) and Gould (1998) also provide evidence of worsening health outcomes and a decline in the urban under-5 mortality advantage which cities usually have.
Historical records of the plague in medieval cities, like the cholera outbreak in the city of London in 1854, and in the early and middle 19th century in the United States, show an increased mortality “penalty” for living in cities (Haines, 2001). Knowledge and sanitary infrastructure could not keep up with the other advantages of urban agglomeration. The delicate balance of food supply, population growth and health in cities foundered in much earlier cases of urban decline. For example, as a result of the 4.2 Kiloyear climate change event around 2,200 BC, aridification led to food shortages and eventually the fall of the first Sumerian cities in Mesopotamia (Christian, 2004).
Whether cities provide an advantage or a penalty for health also depends on people’s age. Dawei Zhu and colleagues (2021) found, for example, that for the middle and early old-age populations in China, the urban health penalty in cities dominates over the urban health advantage; and it returns to an advantage in older ages.
Those dynamics are based on more complex interdependencies between people and environments in cities. They tell us, that although urbanization has often been observed to be associated with better population health, that is only the case, if population growth goes hand-in-hand with other health-related infrastructure improvements, such as sanitary infrastructure, which are underpinned by adequate knowledge and scientific understanding of the interconnections between human health and the environment, including climate change.
The urban advantage, which is largely due to agglomeration and network effects, can only improve human health and wellbeing, if improvements in medical and other sciences, public infrastructure and services, community engagement and intelligent governance keep pace with population growth and physical infrastructure growth (Berggruen and Gardels, 2013). If they do not, disparities and inequalities increase and the urban health penalty begins to dominate. Increasing inequality can be observed to occur “naturally” as societies developed from foraging to farming, became more specialised, more complex, could capture the energy of the sun through agriculture, and eventually had access to an abundance of fossil fuel energy. To reduce social and economic inequalities, government tax policies and transfers are required to drive income inequality down, as initially happened in the OECD countries by 1970 (Morris, 2015; Piketty, 2014).
On this journey of dynamic complexity, cities can be regarded as microcosms of civilisations, which have frequently grown and collapsed in the past, from the first cities in Mesopotamia, following the advent of agriculture, to the “Life and Death of Great American Cities” (Jacobs, 1961).
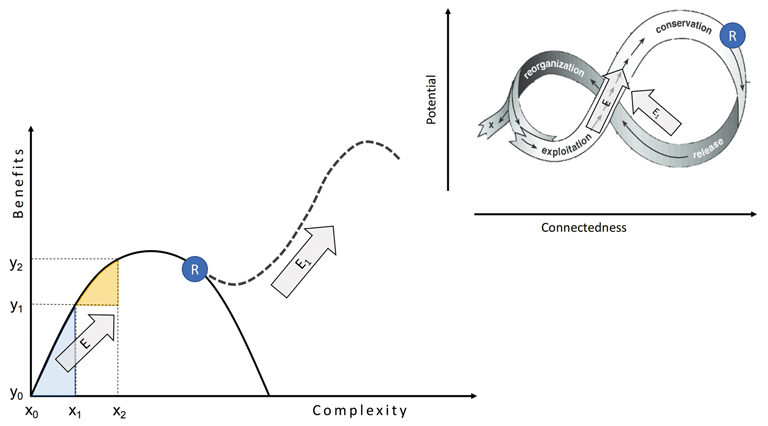
Behind these cycles of growth and decline are network and scaling effects and periods of innovation, which need to occur in ever faster frequencies if collapse can be avoided. Tainter (1988) has described these growth cycles and formulated a law of diminishing returns from increasing complexity (Figure 1). The scaling laws behind these growth cycles apply to physical and biological networks alike (West, 2017). Both, Tainter’s and West’s insights correspond with the adaptive cycle described in the panarchy concept by Gunderson and Holling (2002) and describe the connectedness and potential of complex living systems. The potential of a system can also be understood as its health.
Figure 1: As cities grow and complexity is added, marginal benefits from additional complexity reduce on the same growth trajectory, unless at some point R, innovations occur that transform systems and put them on a new growth trajectory E1.
Figure 1 shows that according to Tainter’s (1988) theory of diminishing marginal returns from increasing complexity, benefits from increasing complexity3 diminish from the beginning towards the end of an exploitation trajectory E. In Figure 1, benefits y2-y1 are smaller than the benefits y1-y0, despite the same amount of additional complexity (x2-x1 = x1-x0). The sub- and super-linear scaling laws in networks (West, 2017) match with that theory, depending on which position (and systemic state) one is on the growth trajectory. As a result of diminishing and decreasing marginal benefits from complexity, the system can collapse, if there are no innovations at some point R, which can trigger a new growth trajectory E1.
Two Lessons from Complexity Science for Urban Health and Wellbeing
Two key lessons from complexity science for improving health and wellbeing in cities are therefore, that we need:
1) An improved systemic understanding of the city as a complex system
The ability to recognise cities as a system of subsystems and determine the systemic state of a city on its trajectory of increasing complexity. The health of people in cities can serve as an indicator for that systemic state, as health is defined as an emergent property from many interconnected social and environmental determinants (Jayasinghe, 2012).
2) Better capacity to identify levers/interventions and formulate policies in response to a city’s systemic state
After analysing and mapping an urban system, an advanced systemic understanding of its components and interconnections will facilitate the choice of policies which are informed by systems science. Policy choices can thereby be less critical, extreme or harmful for urban populations. Policies, which do not increase the risk of system failure or reduce the occurrence of unintended side-effects, become more likely. As “health” is an emergent property of urban systems, integrating health into urban policies is likely to create multiple co-benefits.
For that reason, accelerated learning of systems approaches to urban health and wellbeing is essential. The challenge for future urban health and wellbeing lies in aligning and matching increases in complexity in social, technological and ecological systems. Mismatches and gaps between urban growth and the emergence of corresponding networked infrastructure, are potential avenues for system decline and collapse.
Future cities, especially in the context of globally agreed climate adaptations, such as the 2015 Paris Agreement, will need to accommodate more people aspiring for better standards of living, with simultaneously reduced per capita use of energy and resources.
The urgent conclusion is that ecological and carbon footprints of future cities need to be smaller, and cities need to become more compact, resilient, and sustainable. In order to maintain the urban health advantage under such changing environments, the growth of cities needs to be accompanied by technological and institutional innovations which improve efficiency but also transform towards integrated, networked urban infrastructure innovations (Derrible, 2016). Urban infrastructure systems include, for example, transport or telecommunication infrastructure, energy, sanitation, water, food systems or urban green infrastructure. They are “networked” in the sense that they interact, are interdependent and co-develop.
Examples of innovations in networked urban infrastructure systems include distributed, decentralised power generation, which simultaneously becomes more integrated with transportation and electric vehicles that become energy storing devices during off-peak and provide energy during peak hours (Nourinejad, Chow and Roorda, 2016). In the social domain, multi-level, integrated and participatory governance is emerging, which can be regarded as increasing social system complexity, or a co-adaptation to the increasing coordination needed because of the increasing complexity of other urban systems (Alberti et al., 2019).
Goals and Proposed Actions
In response to those complexity challenges, the new goals of the UHWB Programme focus not merely on creating healthy lives in healthy cities, or making cities more livable and people-centred, rather they aim at solving the core conflict created by an anthropocentric focus on health at the expense of the environment, by putting a focus onto the health of cities, understood as complex urban systems. Accordingly, the goals and action to implement them have been defined by UHWB programme’s scientific committee to comprise the following actions:
Goal 1: Support efforts for implementing Health in All Policies (HiAP) and implement the Xiamen Call for Action in cities.
Actions for goal 1: Collaborate with the InterAcademy Partnership’s working group on urban health to define projects and deliverables for demonstrating how to integrate health in all policies. Liaise with WHO and UN-Habitat and other UN agencies and relevant organisations to identify opportunities of where and how health can be integrated into urban policies.
Goal 2: Lead the development of an interdisciplinary research project on Data-Knowledge-Action Systems for Healthy and Resilient Cities, together with the Committee on Data for Science and Technology (CODATA), and other ISC programmes and organisations.
Actions for goal 2: Draft a concept note and elaborate a proposal for research and action on Urban Data-Knowledge-Action Systems as a cross-cutting theme. Liaise with partners to implement potential demonstration projects.
Goal 3: Communicate the systems approach for urban health and wellbeing to urban decision and policy makers and thereby contribute to a better understanding of complexity governance and health as a global public good.
Actions for goal 3: Together with the International Society for Urban Health, provide workshops/seminars/lectures for urban decision makers and organisations aiming at systemic planning and problem solving of particular urban health issues.
Goal 4: Inform and develop training, education and communication material for natural and social science communities about how to take a systems approach in all health and wellbeing related research in the changing global science context.
Actions for goal 4: Development of a MOOC on A Systems Approach to Urban Health and Wellbeing and other training and information material for specific stakeholder groups on what it means to take a systems approach. Training on collaborative modelling for urban health and wellbeing.
Goal 5: Cooperate with organizations and networks globally in the building of collective intelligence and action for systems approaches to urban health and wellbeing. Consider establishing local and regional chapters of the programme.
Actions for goal 5: Cooperate with WHO Collaborating Centres to produce information & training material on how to take a systems approach and thereby contribute to the regional WHO-WPR strategy. Discuss potential model projects. Build regional communities of practice to link regional development agendas to this UHWB plan.
Conclusions
Despite the site-specific differences between cities in different regions of the world, current global urban trends and the increasing risks they pose to urban and planetary health require us to understand cities as interconnected complex living systems. To grasp the opportunities evident in increasing urban complexity, we must address the emerging challenges for urban health and wellbeing by promoting a new urban systems science and adopting systems approaches for the co-creation of solutions for future healthy cities. There is a wide range of examples at different levels for such solutions inspired by systems thinking, from urban community rooftop gardens, healthy housing in buildings that can generate energy, urban green spaces, networked urban infrastructure, collaborative urban systems modelling, to integrating health into urban and territorial planning at high-level policy making.
The new science plan of the International Science Council’s interdisciplinary programme on “Urban Health and Wellbeing: A Systems Approach” has provided the rationale and background of what a systems approach to health and wellbeing in cities is and why it has become a necessity in the current age of the Anthropocene.
By defining goals and actions, which the programme itself and other urban stakeholders can adopt and adjust to their own specific local requirements and circumstances, our aim is to trigger systems thinking for solutions to promoting urban health and give collaborative guidance for developing solutions in cities around the world. Together with a growing global network of scientists and other urban stakeholders who are exchanging knowledge, we can learn from each other and work together towards these goals that can help to sustainably shape the future of urban health and wellbeing.
References
Alberti, V., et al. 2019. The Future of Cities, Vandecasteele, I., Baranzelli, C., Siragusa, A. and Aurambout, J. editor(s), Publications Office of the
European Union, Luxembourg, doi:10.2760/364135, JRC116711
Antai, D. and Moradi, T. 2010. Urban Area Disadvantage and Under-5 Mortality in Nigeria: The Effect of Rapid Urbanization, Environmental
Health Perspectives, 118(6): 877–884.
Berggruen, N. and Gardels, N. 2013. Intelligent Governance for the 21st Century: A Middle Way between West and East. Cambridge, UK:
Polity Press.
Christian, D. 2004. Maps of Time. Berkeley, LA, London: University of California Press.
Derrible, S. 2016. Complexity in Future Cities: The rise of networked infrastructure, International Journal of Urban Sciences, DOI:
10.1080/12265934.2016.1233075
Gatzweiler F, Bojie Fu, Celine Rozenblat, Huey-Jen Jenny Su, Isaac Luginaah, Jason Corburn, Jo Ivey Boufford, Juan Vela Valdes, Blaise
Nguendo-Yongsi, Philippa Howden-Chapman, R. B. Singh, Rachel Cooper, Tolullah Oni & Yong-Guan Zhu. 2020. COVID-19 Reveals the
Systemic Nature of Urban Health Globally, Cities & Health, DOI: 10.1080/23748834.2020.1763761
Gould, W.T.S. 1998. African Mortality and the New “Urban Penalty”. Health & Place, 4(2): 171–181.
Gunderson, L.H. and Holling, C.S. (eds.) 2002. Panarchy: Understanding transformations in human and natural systems. Washington, London:
Island Press.
Haines, M.R. 2001. The Urban Mortality Transition in the United States, 1800–1940, Historical Working Paper 0134, DOI 10.3386/h0134
IPCC Reports: https://www.ipcc.ch
Jacobs, J. 1961. The Death and Life of Great American Cities, New York: Random House.
Jayasinghe S. 2012. Complexity Science to Conceptualize Health and Disease: Is it relevant to clinical medicine? Mayo Clinic
Proceedings, 87(4), 314–319. https://doi.org/10.1016/j.mayocp.2011.11.018
Kotzé, LJ, and French, D. 2018. The Anthropocene Ontology of International Environmental Law and the Sustainable Development Goals:
Towards an Ecocentric Rule of Law in the Anthropocene, Global Journal of Comparative Law, 7(1):5–36.
Küpers, W.M. 2020. From the Anthropocene to an “Ecocene”, Sustainability, 12, 3633, doi:10.3390/su12093633
Morris, I. 2015. Foragers, Farmers and Fossil Fuels: How Human Values Evolve. Princeton and Oxford: Princeton University Press.
Nourinejad, M., Chow, J. Y. J., & Roorda, M. J. 2016. Equilibrium Scheduling of Vehicle-to-grid Technology Using Activity Based Modelling.
Transportation Research Part C: Emerging Technologies, 65, 79–96.
Piketty, Th. 2014. Capital in the Twenty-First Century. Boston, Harvard University Press.
Tainter, J. A. 1988. The Collapse of Complex Societies. New York, NY: Cambridge University.
Thoradeniya, T. and Jayasinghe, S. 2021. COVID-19 and Future Pandemics: A global systems approach and relevance to SDGs,
Globalization and Health, (2021) 17:59. https://doi.org/10.1186/s12992-021-00711-6
West, G. 2017. Scale: the universal laws of growth, innovation, sustainability, and the pace of life in organisms, cities, economies, and
companies. New York: Penguin Press.
Zhu, D., Ye, X., Li, W., Ding, R., and He, P. 2021. Urban Health Advantage or Urban Health Penalty? Urban-rural disparities in age trajectories
of physiological health among Chinese middle-aged and older women and men. Health and Place, 69, 102559, doi.org/10.1016/
j.healthplace.2021.102559
1 Executive director of the ISC global science programme “Urban Health and Wellbeing: A Systems Approach” at the Institute of Urban Environment, Chinese Academy of Sciences based in Xiamen, China.
2 Chair of the scientific committee for the ISC global science programme “Urban Health and Wellbeing: A Systems Approach” at University of Otago, Wellington, New Zealand
3 Here complexity is defined as increasing network structure of interconnectivity and connectedness and additional functions and urban infrastructure.