With the development of brain chemistry, we now hear more often the word “anhedonia”. What is anhedonia? Psychiatrists define anhedonia as the inability to experience pleasure, to enjoy life. This term appeared in the mid 20th century as one of the major characteristics of schizophrenia.
In fact, anhedonia is a core clinical symptom for various mental disorders including schizophrenia, major depressive disorder, bipolar disorder, and substance abusers. It has been thought to be an important predictor of functional outcome and disease liability. Traditionally, anhedonia was defined as a reduced ability to experience joyful events or an intention to approach rewards. However, recent advances in clinical and affective neuroscience suggested that such a traditional conceptualization of anhedonia as a sole diminished capacity for pleasure may not sufficiently characterize the affective abnormalities that occur in these mental disorders, especially schizophrenia. The beliefs about pleasure may have an important role in articulating the internal experience of pleasure to external observable behavioral deficits of anhedonia, e.g., beliefs that engaging in social interaction is not pleasurable may finally lead one not to take part in any social activities generally. However, there is no available measure for us to capture this kind of belief about pleasure in both clinical and general populations.
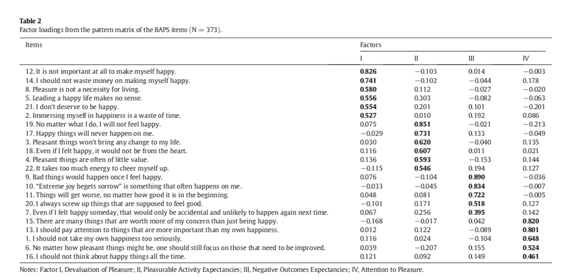
To bridge such a gap of knowledge, Dr. Raymond CHAN from the Neuropsychology and Applied Cognitive Neuroscience Laboratory, CAS Key Laboratory of Mental Health, Institute of Psychology, and the Department of Psychology, the University of Chinese Academy of Sciences, has collaborated with his international colleagues to conduct a series of studies to specifically examine low-belief about pleasure in both clinical and non-clinical samples. In the first study, they developed the Belief About Pleasure Scale (BAPS) and validated it a group of 373 college students. Findings from exploratory factor analysis showed the BAPS items loaded onto four factors, namely the “Devaluation of Pleasure”, the “Pleasurable Activity Expectancies”, the “Negative outcomes Expectancies”, and the “Attention to Pleasure”. These factor scores demonstrated good internal consistency and test-retest reliability at a six-week interval. Moreover, the BAPS also correlated significantly with measure capturing experiential pleasure.
In the second study, they administered the BAPS to a group of 838 patients with schizophrenia and 349 healthy controls.
Confirmatory factor analysis suggested a bi-factor model similar to the four-factor solution in study 1 was replicated. The derived factor scores could discriminate patients with schizophrenia from healthy controls significantly. More importantly, the BAPS total score was correlated significantly with anhedonia subscale of clinical ratings conducted by psychiatrists.
Finally, they further examined whether such a low pleasure belief about pleasure would be demonstrated in individuals across the spectrum of the disorders. In so doing, they recruited 65 patients with first-episode schizophrenia, 65 individuals with social anhedonia, and 65 healthy controls to examine their belief about pleasure. The findings showed that there was a significant difference among the three groups in the BAPS total score and the four BAPS subscale scores. In particular, patients with first-onset schizophrenia reported significantly higher than controls on the BAPS. These patients also reported higher than the individuals with social anhedonia on the BAPS devaluation of pleasure subscale score. On the other hand, the individuals with social anhedonia reported significantly higher than healthy controls on the BAPS total score, and the subscale scores, except the attention to pleasure subscale.
Taken together, these findings provided preliminary evidence for the presence of low-pleasure beliefs in both clinical and subclinical groups and suggested that the BAPS has promising initial psychometric properties. These findings highlight the important of the belief system withheld by patients with anhedonia such as schizophrenia, major depressive disorder, bipolar disorder and substance abusers. The BAPS may serve as a very useful tool to elucidate the efficacy of psychological interventions targeting anhedonia.
Dr. Raymond CHAN’s team is now conducting a cross-cultural study to compare and contrast the reported belief about pleasure in healthy volunteers from different countries. Moreover, they are also examining the underlying neural correlates of such a low-belief about pleasure in both clinical and subclinical samples. They hope to provide a new direction for mental health assessment and intervention for people suffering anhedonia in the near future.
The study was supported by the National Natural Science Foundation of China, the National Key Research and Development Program, the China Postdoctoral Science Foundation funded project, the Beijing Training Project for the Leading Talents in Science and Technology, the Beijing Municipal Science & Technology Commission Grant, the CAS key Laboratory of Mental Health, Institute of Psychology, and the CAS/SAFEA International Partnership Program for Creative Research Teams. (Text by Dr. Raymond CHAN’s team)
